Treatment cascades show 90-90-90 goal within reach for some – but Eastern Europe lags behind Africa 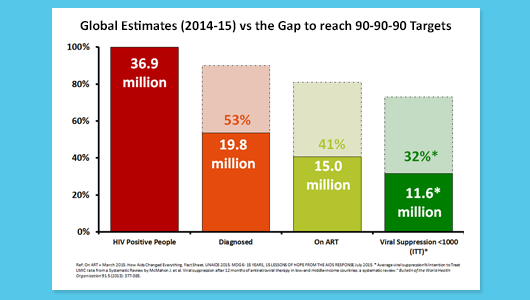
Image from presentation by Jacob Levi, Imperial College London, at IAS
2015. Global analysis
of HIV treatment cascades – the proportions of people diagnosed with HIV, in
care, on treatment and virally suppressed – shows
that some of the world’s richest countries are still far short of achieving the
UNAIDS 90-90-90 target.
Progress is worst in Eastern Europe.
The findings
were presented by Jacob Levi at the Eighth International AIDS Society
Conference on HIV Pathogenesis, Treatment and Prevention (IAS 2015) in Vancouver –
described by numerous speakers this week as the ‘90-90-90’ conference.
The 90-90-90
target set by UNAIDS aims to diagnose 90% of all people with HIV, provide antiretroviral therapy for 90% of those
diagnosed, and achieve undetectable HIV RNA for 90% of those on treatment, by
2020. This ambitious target translates into undetectable viral load in 73% of
all people living with HIV.
How far are countries from
achieving these targets? In some cases fairly close, but in others, the gap is enormous.
Research conducted by a team from
Imperial College, London, and the Cantonal Hospital of St. Gallen, Switzerland,
updating a previous survey, shows that Switzerland, Australia and the United Kingdom have the
highest proportion of people living with HIV with undetectable viral load. In
these countries, over 60% of the estimated population of people living with HIV
have undetectable viral load, compared with 30% in the United States.
Worldwide, 36.9 million people are estimated to be living with HIV of whom 53% are diagnosed, 13.4 million people short of the 90% target. 41% are on treatment, 14.9 million people short of the target, and 32% are virally suppressed, 15.3 million people short of the target. Approximately 2 million people each year are becoming infected at current rates of transmission.
Breaking this down to look at
national treatment cascades, the research group found enormous variations at
each stage of the cascade. They sought to identify ‘breakpoints’ – steps where
more than 10% of people were lost.
The proportion of the estimated
population of people living with HIV who had been diagnosed varied from 86% in
the United States and Australia to 51% in sub-Saharan Africa and 44% in
Ukraine. Many countries were identified as having breakpoints in HIV diagnosis,
indicating the global importance of improving rates of HIV diagnosis.
Cash to stay in school doesn’t reduce HIV incidence in South African study – but school attendance protected young women against HIV 
HPTN 068 study team. Image supplied by Audrey Pettifor.
Education has
been shown to have a protective effect against HIV infection in sub-Saharan
Africa, especially for young women. Interventions to promote school attendance
are being explored in several countries, including the use of cash transfers to
encourage school attendance. Two large randomised studies reported results
this week at the conference.
A conditional
cash transfer to the households of adolescent girls to promote school
attendance did not reduce HIV incidence in a randomised study in rural South
Africa, Audrey Pettifor of the University of North Carolina reported.
Although
receipt of the cash transfer was not associated with reduced HIV incidence, it
was associated with a lower rate of unprotected sexual intercourse compared to
a control group.
The study also
found that dropping out of school, or poor school attendance, was associated
with a significantly higher rate of HIV incidence in young women. The finding
confirms observations in several African countries which show that education
has a protective effect against HIV infection both during the school years and
afterwards for young women.
A second study,
CAPRISA 007, showed that a conditional cash transfer to young women and men
tied to HIV testing, participation in life skills training and academic
attainment, reduced the incidence of HSV-2 (herpes simplex virus-2) by 30% but
did not have an impact on HIV incidence.
…but cash incentives do promote uptake of male circumcision and PMTCT services 
Image from presentation by Harsha Thirumurthy, at IAS 2015. Cash
incentives are also being explored as a means of promoting uptake of prevention
services. Cash compensation can improve the uptake of key HIV prevention
services in sub-Saharan Africa, results from two randomised studies show.
A randomised
trial conducted in Nyanza province, Kenya, showed that offering compensation in
the form of food vouchers resulted in a significantly higher uptake of medical
male circumcision. A second randomised trial conducted in the Democratic
Republic of the Congo showed that providing modest cash incentives
significantly increased retention in services for prevention of mother-to-child
HIV transmission (PMTCT).
Pre-exposure prophylaxis (PrEP) 
PrEP symposium panel at IAS 2015. Photo by Liz Highleyman, hivandhepatitis.com. How to take PrEP and what
people think about taking PrEP
have been the subjects of much discussion at the International AIDS Society
conference.
Two large
studies, ADAPT (HPTN 067) and Ipergay, have shown that it is possible for
people to take intermittent PrEP regimens so that most episodes of sex are
covered by PrEP. This should provide protection against infection, but
pharmacological information is needed to be confident that people are achieving
adequate drug levels of the components of Truvada
(emtricitabine and tenofovir) when they are actually taking PrEP.
A pharmacological sub-study of the PrEP
regimen used in the Ipergay study was presented on Monday. Participants in Ipergay took two doses
before sex and two doses after sex. The study indicated that in men who have
sex with men (MSM) taking the regimen, emtricitabine begins to provide
protection within 30 minutes of dosing but tenofovir takes 24 hours to reach
adequate levels in rectal tissue. This means the post-sex doses are especially
important in people who use PrEP less than once or twice a week.
Another
pharmacological study showed that intermittent dosing may provide less adequate
drug levels for protection of women during vaginal sex, because tenofovir took
twice as long to reach peak levels in the cervix as in the rectum – and only
ever achieved 10% of rectal tissue levels in the cervix.
In terms of
protection from transmission via anal intercourse, the researchers calculated
that 77% protection against HIV was reached after one dose of tenofovir. This
is higher than the 38% suggested by a rectal explant study (using tissue samples in a laboratory), though the lower
bound of the confidence interval in this study is 40%. Estimated protection is
89% after two doses, and 98% after three: a
previous sub-study of the iPrEx PrEP study concluded that four doses a week would be enough to offer
essentially 100% protection from HIV.
What does this
tell us about the protectiveness of the Ipergay regimen – and of the
intermittent regimens in ADAPT?
Firstly, we
still do not know enough about protection in vaginal and cervical tissues to
say whether or to what degree intermittent PrEP would be effective for women,
or trans* men who have vaginal sex. At present, it is therefore best to
recommend daily dosing for vaginal sex.
For anal sex,
however, it does look as if significant protection lasts anything up to a week
after the previous dose of PrEP, if people have been taking it steadily. It would
be rapidly ‘topped up’ by the emtricitabine within hours of a subsequent double
dose as long as the interval was no longer than that. If PrEP is taken
before sex but after a long time gap, however, the post-sex doses – both of
them – are very important to take too.
In this
context, it is notable that the Ipergay regimen offers much greater timing
flexibility, as the first post-sex dose can be taken any time in the next 24
hours; this is much easier than taking it two hours after sex, something the ADAPT participants found
difficult.
The reasons whether or not people come forward for PrEP or take it once prescribed are likely to be very mixed, and dependent as
much on local political and cultural beliefs as they are on more personal
factors like relationship status.
Serosorting and viral load 
Image from Opposites Attract study. www.oppositesattract.net.au ‘Serosorting’
refers to the practice of people choosing sexual partners they perceive to have
the same HIV status as themselves, or of choosing not to use condoms with such partners.
But it is clear that the scenarios are not necessarily as simple as HIV-negative
people pairing up with other HIV-negative people, or of HIV-positive people
sticking with HIV-positive people.
Gay men may
decide which partner takes the receptive (‘bottom’) role dependent on each
man’s HIV status. An HIV-negative person may consider that having condomless
sex with an HIV-positive person who has an undetectable viral load is safer
than doing so with someone who claims to be HIV-negative but last tested a year
ago. But engaging in these ‘sero-adaptive’ behaviours depends on individuals’
and communities' level of understanding of HIV transmission factors and can
also be limited by HIV stigma.
There is
evidence that some groups of Australian and American gay men are considering
HIV-positive partners’ undetectable viral load and the time elapsed since an
HIV-negative partner last tested when making decisions about using condoms, according to studies presented to the conference.
The findings suggest that as
community discussion and awareness about viral load and transmission risks when
viral load is undetectable grows, discussion about viral load begins to
influence decisions about condom use, and thinking about the HIV status of
partners becomes more sophisticated.
Couples counselling 
Image
from presentation by Dr Nora Rosenberg, at IAS 2015. In Malawi, HIV counselling and
testing for pregnant women is close to 100%. Although couples counselling and
testing is encouraged, male partners rarely come forward and an opportunity for
HIV diagnosis is missed.
When couples are counselled and
test for HIV together, there are potential benefits. These include having the
opportunity to make informed decisions about HIV prevention and reproductive
health together, mutual support and improved adherence to treatment. Lack of
male involvement is often cited as a barrier to women accessing treatment and
care, including prevention of mother-to-child transmission interventions.
Researchers in Lilongwe, Malawi,
investigated whether actively contacting male partners of women accessing
antenatal care could increase uptake of couples HIV counselling and testing.
They tested two
options – sending an invitation to male partners; and sending an invitation and
following it up with a phone call or home visit.
Both strategies resulted in men
coming forward for counselling and testing, with the ‘invitation plus tracing’
strategy substantially increasing the uptake of couples counselling and
testing. Of 126 men who came forward, 47% tested positive for the first time
(an additional 25% already knew they had HIV). Dr Rosenberg, presenting the study, suggested
that this strategy could have important public health benefits.
New ARVs: a promising maturation inhibitor could offer a new drug class 
Carey Hwang at IAS 2015. Photo by Liz Highleyman, hivandhepatitis.com Combination antiretroviral therapy (ART) consists of agents that target
different steps of the HIV lifecycle, but none of the currently approved drugs
inhibit viral assembly, maturation and release from host cells.
The next-generation HIV maturation inhibitor BMS-955176 was
well-tolerated and suppressed HIV viral load as well as standard
antiretrovirals when used in a combination with atazanavir (Reyataz) in
a 28-day study, according to late-breaking results
presented at the conference.
If further studies confirm its safety and efficacy, BMS-955176 could be
the first drug in a new class of antiretrovirals that may offer an important
treatment option for people with HIV who have developed extensive resistance to
existing drug classes.
|






Connect with NAM on Facebook: Keep up to date with all the exciting projects, latest achievements and new developments that are going on in the world of NAM.
Follow NAM on twitter for links to hot off the press news stories from our editors covering key developments and conferences as they happen. Our news feed is linked to www.twitter.com/aidsmap_news and we also tweet from www.twitter.com/aidsmap.
Follow all the conference news by subscribing to our RSS feeds.